 AIDS
and Dementia
AIDS
and Dementia
By Dana Gabuzda, M.D.
AIDS
and Dementia
By Dana Gabuzda, M.D.
One devastating complication of AIDS is a dementing illness caused by HIV infection of the brain. This disorder, which eventually affects as many as 20 to 30 percent of AIDS patients, causes a spectrum of neurological and psychiatric symptoms. These range from mild cognitive impairment to a severe dementing disorder referred to as AIDS dementia. Less frequently, HIV can also cause other neurological disorders such as damage to sensory and motor nerves and spinal cord degeneration. AIDS dementia is distinct from brain infections by opportunistic microorganisms and brain lymphoma which can also occur in AIDS patients due to the weakened immune system.
HIV infection of the brain occurs early after initial exposure to the virus, probably within the first few months. However, the infection remains clinically silent over many years; most HIV-infected individuals do not develop cognitive symptoms until many years later, after the onset of full-blown AIDS.
The initial trigger that causes the emergence of AIDS dementia in some patients after years of silent brain infection is unknown. One key factor may be the development of certain "neurovirulent" HIV strains due to genetic changes in the virus within an individual who has been infected with HIV for many years. Other factors may relate to the gradual increase in total virus load within an infected individual over time, leading to increased levels of potentially neurotoxic factors produced by the virus or infected cells.
The initial symptoms of AIDS dementia are usually mild and occur gradually. The early symptoms may include memory loss, impaired mental concentration, and slowness in performing mental tasks. For example, affected individuals may feel less quick in their thinking or notice that they lose track during conversation or while reading. Family members and friends may notice behavioral abnormalities, such as personality changes, loss of interest in activities, or social withdrawal. Depression is another common symptom. However, depression can also be caused by the psychological stress of HIV infection and is not invariably attributable to AIDS dementia. Individuals whose cognitive symptoms remain relatively mild may experience little impairment. However, in more severely affected individuals, the disorder may progress relentlessly over several months, leading to marked cognitive impairment and significant neurological disability. In the advanced stages, patients can also develop weakness, tremor, rigidity, and seizures.
Important clues about the disease processes that cause AIDS dementia have come from studies of autopsy brain tissue. AIDS brain tissue frequently shows evidence of a pathological process called "HIV encephalitis," even in individuals who had no neurological symptoms. The brain shows areas of low-grade inflammation and damage to myelin, the coating on nerve cells' projections. These abnormalities are accompanied by nerve cell loss, which can be as high as 18 to 30 percent in severely affected brain regions.
Nerve cell loss is likely to be the direct cause of AIDS dementia. However, the disease processes that ultimately lead to nerve cell death probably begin with progressive damage to several different brain structures. The most severely affected brain structure is the basal ganglia, a region deep in the brain that is involved in regulating certain motor and cognitive functions. Another greatly affected structure is the white matter, which contains supporting cells and nerve cell myelin, which is necessary for the efficient and rapid conduction of nerve signals.
The cerebral cortex -- the folded outer layer of the brain which contains the nerve cells responsible for most cognitive activity -- is also commonly affected. Blood vessels in the brain are also damaged, impairing their ability to block potentially harmful molecules in the blood from entering the brain.
HIV initially enters the brain by passage of HIV-infected cells from the blood. In 1986, our laboratory and other groups demonstrated that the major brain cell types infected by HIV are "macrophages," a type of immune cell, and "microglia," a particular type of macrophage found only in the brain. More recently, studies have shown that other types of brain cells that may become infected at very low levels are astrocytes, which are supporting cells, and endothelial cells, the cells lining the walls of blood vessels.
Nerve cells are not directly infected by HIV, suggesting that nerve cell death is a response to toxic factors released from the virus itself or by neighboring cells. Several potential candidates for the AIDS dementia neurotoxin(s) have been identified, but it remains uncertain which factor is the true culprit.
One potential candidate is gp120, the HIV coat protein (which is just what it sounds like: the protein that surrounds the virus like a coat); gp120 has significant neurotoxic activity in cultured brain cells and animal models. Another candidate, the HIV "Tat" protein, also has neurotoxic activity. Other candidates include potentially neurotoxic factors released by HIV-infected macrophages and microglia. Given the complexity of the virus-host interactions involved in the disease process, it seems likely that more than one of these factors (and probably other, unknown factors) act in concert to cause nerve cell injury.
To learn how HIV causes nerve cell death and to test potential therapeutic agents, our laboratory recently developed a cell culture model for HIV infection of human brain cells. Using this model, we found that only certain strains of HIV could infect human brain cells. As expected, the brain cells that became infected were the macrophages and microglia, which in turn became enlarged and "activated."
Importantly, in this "activated" state, HIV-infected macrophages and microglia have been shown to secrete several potentially neurotoxic factors. These include "tumor necrosis factor a" (TNF-a) and other immune factors; small molecules called "excitotoxins" that can lead to nerve cell death by excessive stimulation of nerve cell activity; and nitric oxide, another potential neurotoxin which has been implicated in other neurodegenerative disorders.
We then examined the effects of HIV infection on nerve cells in culture and found that HIV infection induces nerve cell death by apoptosis (see photo below).
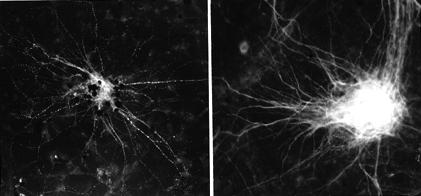
Nerve cell "suicide" (black dots) in HIV-infected huma brain cultures (left). Nerve cells in uninfected cultures appear healthy (right). (Courtesy of Dr. Gabuzda.)
Apoptosis is a cell suicide program that is believed to have a healthy function until it is set off by a disease process such as stroke and Alzheimer's disease, in which it has been implicated. Apoptosis is also a cause of immune cell death in AIDS, raising the possibility that HIV-related damage to the immune system and nervous system may share common mechanisms.
Apoptosis is activated by certain cell proteins and genes, some of which have been identified. Recent studies have identified drugs that can block specific steps in the cell suicide program, providing hope that inhibiting nerve cell apoptosis may be a potential therapeutic approach for AIDS dementia and possibly other neurodegenerative disorders. The human brain cell culture model developed in our laboratory may therefore be a useful tool for discovering drugs that can prevent HIV-induced nerve cell suicide.
We also examined brain tissue from AIDS patients and confirmed that nerve cell apoptosis occurs in the brains of patients with AIDS dementia, a finding recently reported by several other groups. We found evidence of nerve cell apoptosis in some AIDS patients without neurological symptoms, suggesting that the neurodegenerative process may start prior to the development of overt cognitive impairment.
These studies, performed by Dr. Bin Shi, in our laboratory, and collaborator Dr. Umberto DeGirolami, demonstrated that nerve cells undergoing apoptosis were usually not directly adjacent to HIV-infected microglia, suggesting that apoptosis is likely to be induced by factor(s) acting at a distance and diffusing to affect nerve cells. In short, our studies suggest that HIV-infected microglia release neurotoxic factors which then act at a distance to induce nerve cell suicide.
AIDS dementia is a potentially treatable disorder. The antiviral drug AZT significantly improves neurological function in adults and children with AIDS dementia and other HIV-related neurological disorders, but loses efficacy over time due to the emergence of AZT-resistant virus. Clinical trials of other drugs are in progress, including drugs that block the neurotoxic effects of the HIV coat protein gp120. Ultimately, the successful development of drugs to treat or prevent AIDS dementia will depend on improved antiviral therapy and a better understanding of the complex disease processes which cause nerve cell suicide in HIV infection. *
Dr. Gabuzda is an Assistant Professor of Neurology at Harvard Medical School and Dana-Farber Cancer Institute.
![]() Next
Next
![]() Back
to the AIDS Dementia Index
Back
to the AIDS Dementia Index
![]() Home
Home