 Dementia
With Lewy bodies
Dementia
With Lewy bodies
This
text has been compiled with the help of Dr. Graham Lennox
Dementia with
Lewy bodies is a preferred term which describes several common disorders
causing dementia. In many hospitals this is the second commonest cause
of dementia after Alzheimer's disease. The name for the disease comes from
the presence of abnormal lumps which develop inside nerve cells called
Lewy bodies. Following increasing pathological recognition, core clinical
diagnostic features have been identified to allow diagnosis in life.
These diseases have been given a variety of names by different workers.
- Diffuse Lewy
body Disease
- Cortical
Lewy body Disease
- Lewy Body
Dementia
- Senile Dementia
Of Lewy Type
- Lewy Body
Variant of Alzheimer's Disease
The main features
of these conditions are
- development
of dementia with features overlapping with those of Alzheimer's disease
- development
of features of Parkinson's disease
- fluctuation
in severity of condition on a day-to-day basis
- Early development
of hallucinations
PATHOLOGICAL
FEATURES
Several key
areas of the brain undergo degeneration in this form of disease
- There is
degeneration of an area in the brain stem called the substantia nigra as
would be seen in Parkinson's disease. Normally the substantia nigra is
populated by nerve cells which contain a dark-brown pigment called neuromelanin.
The cells of the substantia nigra are responsible for making the neurotransmitter
dopamine. In both Parkinson's disease and Lewy body dementia these cells
die and so the substantia nigra appears abnormally pale in comparison to
normal. Remaining nerve cells contain abnormal structures called Lewy bodies.
which are a pathological hallmark of the disease process.
- Degeneration
of the cortical areas of the brain with many or all of the features seen
in Alzheimer's disease
- Degeneration
of the cortical areas of the brain with formation of abnormal structures
inside nerve cells called cortical Lewy bodies which can be detected by
immunochemical staining for the protein ubiquitin.
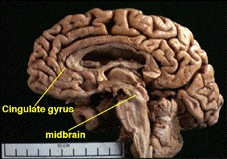
When the brain
from a patient with Lewy body dementia is examined at autopsy loss of nerve
cells is seen from the midbrain region where the substantia nigra is located.
Shrinkage of the brain is particularly seen in the temporal lobe, and parietal
lobe.
PATHOLOGICAL
FEATURES ASSOCIATED WITH DLB
- Essential
for diagnosis of DLB
- Associated
but not essential
- Lewy-related
neurites
- Plaques (all
morphological types)
- Neurofibrillary
tangles
- Regional
neuronal loss - especially brain stem (substantia nigra and locus coeruleus)
and nucleus basalis of Meynert
- Microvacuolation
(spongiform change) and synapse loss
- Neurochemical
abnormalities and neurotransmitter deficits
CLINICAL
FEATURES AND DIAGNOSIS OF DLB
The core feature
of DLB is a progressive dementia.
- Clinically,
this condition can present as a dementia which is often initialy diagnosed
as either Alzheimer's disease or vascular dementia.
- Alternatively,
many patients start with classical Parkinson's disease and later go on
to develop dementia.
- Only a minority
of patients present with the simultaneous onset of both dementia and parkinsonism
A combination
of key clinical features has allowed workers in many centres to diagnose
this condition and distinguish it from other causes of dementia.
- Most patients
initially complain of impaired recent memory.
- In other
patients the main problem is behavioural disturbance with preserved memory.
- Speech block,
problems with word-finding, problems in following an unfamiliar route may
happen early in the disease.
- Features,
such as inattention, mental inflexibility, indecisiveness and lack of judgement,
together with loss of insight, may also develop in the early stages of
the disease and are useful in suggesting the possibility of a non-Alzheimer
form of dementia.
- An important
feature which helps to distinguish DLB from Alzheimer's disease is the
presence of striking fluctuations in cognitive performance during the early
stages of the disease. By way of example, one day a patient may be able
to hold a sustained conversation, the next they may be drowsy, inattentive
and almost mute. Some patients have periods of frank stupor, which often
causes clinicians to search (in vain) for an intercurrent diseases such
as infection or stroke. The basis of these fluctuations is not clear.
- Another very
characteristic clinical feature is the presence of visual hallucinations.
The hallucinations are typically complex and detailed. For example, patients
may see images of people or animals that they recognise. Some patients
see coloured patterns or shapes. Interestingly, the hallucinations are
not always distressing to patients and many learn to distinguish between
real and unreal images: some people actually come to enjoy them. In many
patients visual hallucinations are accompanied by delusions which tend
to have a persecutory theme.
- A third characteristic
clinical feature is the presence of clinical features of parkinson's disease.
These develop spontaneously in most patients who have initially presented
with dementia, and may be relatively mild. The typical features are
- a flexed
posture
- a shuffling
gait
- reduced armswing
- a tendency
to falls.
- a paucity
of spontaneous movement
- Tremor is
the least common parkinsonian feature in patients who have presented with
dementia.
- Patients
with DLB are often abnormally sensitive to neuroleptic therapy, developing
parkinsonism even if they have not shown such signs before drug administration.
The associated parkinsonism is often prolonged, profound and may even be
fatal.
- In almost
all patients disease is relentless and progressive: the dementia becomes
global and severe. Eventually patients become profoundly demented and immobile,
and usually succumb to pneumonia or intercurrent illness after an average
of 7 years from the onset of symptoms.
- A small proportion
of patients have a rapidly progressive illness, becoming profoundly demented
within months.
- A minority
of patients start their disease with typical levodopa responsive Parkinson's
disease and later go on to develop dementia.
- This sequence
of events is commoner in older patients and accounts for 30% of patients
overall.
- Typically
cognitive decline starts with depression or mild forgetfulness.
- Many patients
then go on to develop visual hallucinations or delusions which appear to
be related to their anti-parkinsonian therapy.
- These problems
often resolve once anticholinergic drugs or dopamine agonists are withdrawn,
only to recur months or years later as the dementing process becomes more
severe.
- Depression
can complicates clinical assessment and may make the cognitive impairment
seem more severe than it really is.
CLINICAL
DIAGNOSTIC CRITERIA
Clinical diagnostic
criteria have recently been assembled at a recent Consortium meeting to
produce a new set of criteria (McKeith et al, 1996).
- The central
requirement is progressive cognitive decline of sufficient magnitude to
interfere with normal social or occupational function. Prominent or persistent
memory impairment may not necessarily occur in the early stages but is
usually evident with progression.
- Two of the
following are required for a probable, and one for a possible diagnosis
of dementia with Lewy bodies:
- Fluctuating
cognition with pronounced variations in attention and alertness
- Recurrent
visual hallucinations which are typically well-formed and detailed
- Spontaneous
motor features of parkinsonism
- Features
supportive of the diagnosis are:
- Repeated
falls
- Syncope or
transient loss of consciousness
- Neuroleptic
sensitivity
- Systematised
delusions
- Hallucinations
in other modalities
- A diagnosis
of dementia with Lewy bodies is less likely in the presence of:
- Stroke disease,
evident as focal neurological signs or on brain imaging
- Evidence
on physical examination and investigation of any physical illness or other
brain disorder sufficient to account for the clinical picture
CLINICAL
INVESTIGATIONS
There are
no specific diagnostic tests for DLB.
- Detailed
psychometry may help confirm the clinical impression of the pattern of
dementia
- Routine blood
tests are normal.
- Structural
brain imaging with CT or MRI may show generalised cerebral atrophy, sometimes
with a discernible frontal predominance
- Electroencephalography
typically reveals generalised slowing of background activity; occasional
patients with rapidly progressive dementia will show periodic complexes
reminiscent of CJD.
- Brain biopsy
is not routinely justified in suspected cases of DLB.
DIAGNOSTIC
PROBLEMS
In most patients
the main diagnostic issue is to distinguish DLB from the commoner Alzheimer's
disease (AD).
- The presence
of fluctuations, hallucinations and spontaneous parkinsonism all have value
in suggesting a diagnosis of DLB
- To a lesser
extent, frequent falls and severe neuroleptic-induced parkinsonism also
point to DLB rather than AD.
- All of the
above features can sometimes happen in patients with AD occurring either
alone or in combination with brainstem Lewy body Parkinson's disease.
A more common
diagnostic error is to attribute the clinical features of DLB to cerebral
vascular disease such as multi-infarct dementia or Binswanger's disease.
- CT or MR
imaging frequently reveal mild and essentially incidental vascular disease
which can lure the clinical towards a diagnosis of multi-infarct dementia.
- CT or MR
imaging often show diffuse subcortical white matter changes in degenerative
diseases such as DLB, and these can be so striking as to lead to a radiological
diagnosis of Binswanger's disease.
MANAGEMENT
AND THERAPY
There is no
specific therapy that can stop the process of neurodegeneration in this
form of dementia.
Therapy is
limited to managing neuropsychiatric disturbances and the associated movement
diosorders.
DLB causes
several clinical problems with management. There are conflicting requirements
in trying to treat the neuropsychiatric disturbance as well as the parkinsonism
such that treatments for hallucinations, delusions and behavioural disturbance
tend to make the movement disorder worse and vice versa.
Small scale
studies suggest that the newer atypical neuroleptics such as clozapine
and olanzapine may be able to treat psychotic symptoms without precipitating
excessive parkinsonism.
These drugs
may even be successful in treating hallucinations and delusions in patients
with Parkinson's disease who are starting to dement. This would be a great
advantage, because the traditional management involves the withdrawal of
anti-parkinsonian medication, a process which often leaves the patient
lucid but immobile. It is still reasonable to try to simplify anti-parkinsonian
medication as a first step, particularly withdrawing drugs of lower potency
(and particular tendency to cause confusion) such as anticholinergics and
selegeline; where possible dopamine agonists should also be withdrawn,
leaving most patients on levodopa alone.
Some studies
in this area of therapy advise caution.
Neuroleptic
sensitivity in dementia with Lewy bodies and Alzheimer's disease. (Lancet
Vol 351 4 April 1998 pages 1032-33) Authors: Clive Ballard, Janet Grace,
Clive Holmes.
The research
letter to the Lancet is from the Newcastle group.
McKeith and
colleagues originally reported that about half of all patients with Dementia
with Lewy bodies (DLB) exposed to neuroleptic drugs experienced a severe
adverse drug reaction which included deterioration in cognitive function,
parkinsonism, drowsiness and some features of so-called neuroleptic malignant
syndrome. Such patients has a three fold increase in mortality compared
to those not exposed to such drugs (McKeith et al BMJ 1992; 305: 673-678).
This may also occur in association with atypical neuroleptic drugs (McKeith
et al Lancet 1995; 346: 699)
In the study
that they now report in the Lancet the group have looked at the incidence
if neuroleptic sensitivity in a group of 80 patients, 40 with pathologically
confirmed Alzheimer's disease and 40 with pathologically confirmed DLB.
- 53% of DLB
patients were given neuroleptics
- 38% of AD
patients were given neuroleptics
- 29% of DLB
patients had a definite severe sensitivity reaction to neuroleptics. No
severe reactions were seen in the AD group.
- 10% of the
DLB patients had a mild sensitivity reaction to neuroleptics. Mild sensitivity
reactions were seen in 47% of the AD group.
- Severe sensitivity
reactions were seen in DLB patients despte low doses and the use of newer
neuroleptics (47% of the neuroleptics used were newer, atypical compounds).
- All severe
reactions happend within 2 weeks of neuroleptic administration or a dose
change and were associated with a reduction in survival.
The authors
make the following two recommendations:
- Before use
of neuroleptic agents in patients with dementia other pharmacological and
psychological therapies should be explored first.
- If it is
felt that there is no option but to use neuroleptic therapy in patients
with DLB this should be done in the context of a hospital setting under
close monitoring, either in the first week of therapy or after a dose change.
The pharmaceutical
industry is starting to recognise that the cognitive impairment of DLB
may, because of its neurochemical differences, be more amenable to drug
therapy than Alzheimer's disease.Initial anecdotal experience with cholinergic
therpy in DLB has shown some promise.
THE
CAUSE OF DLB
The cause
of this form of neurodegenerative disease is uncertain. There are overlaps
between Alzheimer's disease and Parkinson's disease. Genetic studies are
making some progress in revelaing a matrix of different genes which may
contribute to development of DLB. This appears to be complex but may explain
firstly the relationship of DLB to the other primary Lewy body disorders
including Parkinson's disease and secondly the association with Alzheimer's
disease. It remains to be seen whether genetic testing will be sufficiently
simple to help in clinical diagnosis.
 Back
To Lewy Directory
Back
To Lewy Directory
Back
To Other Dementia Directories